She wakes at three in the morning already damp through her t-shirt, kicks the blanket to the floor, and lies there waiting for the heat to pass. By the time it does, sleep has slipped somewhere out of reach. So she reaches for her phone instead, and types the question a lot of women type in that same dark room: progesterone or estradiol, which one is she supposed to be asking her doctor about?
It is a reasonable question to ask at 3 a.m. It is also, as it turns out, a little bit the wrong one. Progesterone and estradiol are not two brands competing for the same job. They are two different tools, built for two different parts of the same problem, and in a lot of menopause care they are prescribed together for exactly that reason. Neither one replaces the other. The better question, the one that actually gets you somewhere, is which hormone is suited to which goal, and whether you need one of them, the other, or, more often than people expect, both.
Here is a way to think about it that keeps the two straight: one hormone reacts to what is happening to you right now, and the other quietly stands guard over what could happen later. Estradiol shows up for the fire. Progesterone shows up for the fireproofing. Both are prescription medications, estradiol is a prescription estrogen and oral micronized progesterone is FDA-approved under the brand name Prometrium [1], and the job of matching either one to your body belongs to a clinician, not to a search bar at 3 a.m.
What the evidence actually says, goal by goal
Lay the research out goal by goal, and the picture sharpens fast.
Hot flashes and night sweats. This is estradiol’s job, and it is not a close contest. The Endocrine Society’s 2015 clinical practice guideline on treating menopause symptoms names menopausal hormone therapy the most effective treatment for vasomotor symptoms, and says that for most symptomatic women under 60 or within ten years of menopause, the benefits can outweigh the risks when there is appropriate screening [5]. Progesterone is not the agent doing that work. If the woman from that 3 a.m. scene is chasing relief from the heat itself, the estrogen is where the science points.
Protecting the uterine lining. Here the story flips, and this is the row that matters most if you still have a uterus. Estrogen, the very hormone that quiets hot flashes, also stimulates the endometrium to grow, and left unchecked that growth can become endometrial hyperplasia, a precancerous thickening. Progesterone is the counterweight. The PEPI trial, published in JAMA in 1996, put this to a randomized test: estrogen alone produced a large excess of endometrial hyperplasia, while adding a progestogen, including cyclic oral micronized progesterone at 200 mg a day for 12 days a month, kept hyperplasia rates close to placebo [2]. That result is written directly into the FDA label, which lists prevention of endometrial hyperplasia in women on estrogen as an approved use of progesterone [1].
Sleep. A smaller edge, but a real one, and it belongs to progesterone. A 2021 systematic review and meta-analysis in the Journal of Clinical Endocrinology & Metabolism looked at randomized trials of micronized progesterone, mostly in postmenopausal women, and found improvements in several aspects of the sleep cycle and self-reported sleep, though not across every measure tested [3]. It is a modest finding attached to a specific population and setting, not a case for treating progesterone as a general-purpose sleep aid, but the woman lying awake after her hot flash passes does have a documented reason to bring sleep up with her prescriber.
Vaginal dryness and irritation. Back to estradiol, this time in its local form. A Cochrane review of intravaginal estrogen preparations found they relieve symptoms of vaginal atrophy compared with placebo, with no clear difference in effectiveness between creams, tablets, and rings [6]. Progesterone is not the tool for this particular discomfort.
Available as an FDA-approved oral product. Here, honestly, it is a tie. Oral micronized progesterone is approved as Prometrium [1], and estradiol exists in multiple approved oral and other formulations. Neither hormone has a monopoly on legitimacy.
Used by itself in a woman with a uterus. This is the row that resolves the whole debate. Estradiol alone is not considered safe in that situation, because of the endometrial risk described above [2]. Progesterone alone is not typically used for menopause symptom relief either. The honest answer in this row is neither, together.
Line those six answers up, and only one of them looks like a genuine head-to-head contest, and even that one, hot flashes, has a clear winner. Everywhere else the two hormones are doing separate jobs, and in the row that matters most for anyone with a uterus, they are not rivals at all. They are a pair.
The part a scorecard alone would hide
It would be misleading to stop at “who wins which category,” because the two hormones do not weigh the same on the risk side of the ledger, and that imbalance is part of matching the hormone to the goal.
Estradiol is the heavier intervention. Systemic estrogen is powerful medicine, and the large body of hormone-therapy research, including the Women’s Health Initiative trials, is why the Endocrine Society guideline frames hormone therapy around a woman’s age, her time since menopause, and individualized risk screening, and explicitly cautions against using it to try to prevent chronic disease like coronary heart disease or dementia [5]. Progesterone’s risk profile in menopause care is largely tied up with the fact that it is usually taken alongside estrogen, which is part of why the combination gets evaluated as a whole rather than hormone by hormone.
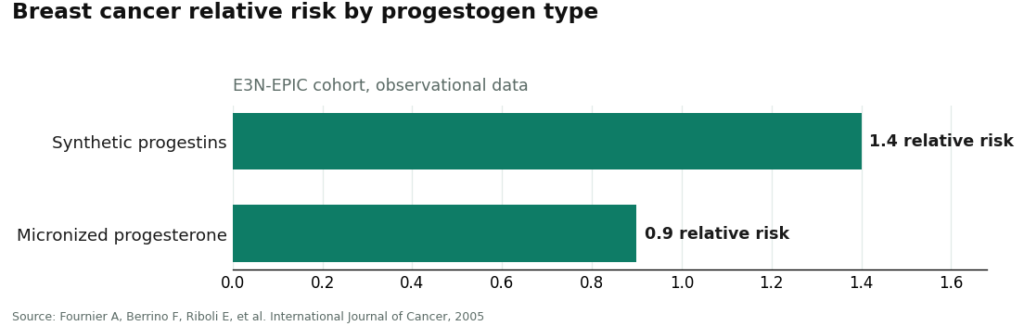
The type of progesterone in that combination turns out to matter too. A cohort study out of the French E3N-EPIC project, published in 2005, compared women on different types of hormone therapy and found breast cancer relative risk running around 1.4 for those on synthetic progestins, versus around 0.9 for those on micronized progesterone [4]. It is observational data, not a randomized trial, so it should be read as one data point rather than a verdict, but it is a reminder that “progesterone” is not a single interchangeable ingredient any more than “estrogen” is a single interchangeable ingredient. The form matters.
The paperwork question that applies to both hormones
There is one more thing worth knowing before anyone fills a prescription: how the product got made. Both progesterone and estradiol come in FDA-approved forms, oral micronized progesterone as Prometrium [1] and estradiol across several approved formulations, and both also circulate in compounded “bioidentical” versions. The same caveat applies to either hormone in its compounded form: compounded preparations are not FDA-approved, and the agency does not review them for safety, effectiveness, or quality before they reach a patient [7]. That does not make a compounded form wrong, there are legitimate clinical reasons a prescriber might choose one, but it is a different regulatory category than the approved product, and a trustworthy provider tells you plainly which one you are getting, for each hormone, rather than letting the word “bioidentical” blur the two together.
This is where the structure of care starts to matter as much as the chemistry. Because the right answer for most women with a uterus is both hormones, dosed and formed to fit the individual, the sensible model is a supervised one: a licensed clinician assesses the person in front of them, chooses the estradiol form and the progesterone form on clinical grounds, weighs the combined risk picture, and a licensed pharmacy fills both. FormBlends is one telehealth provider built on that structure, offering the FDA-approved oral progesterone capsule alongside compounded options, and labeling each honestly for what it is. Nothing here is a sales pitch, and there is nothing to click through to buy. The point is simply that pairing two hormones correctly, at the right doses, is a job for someone trained to weigh them together, not a decision to make from a search result at three in the morning.
Where this actually leaves the woman in bed at 3 a.m.
She does not need to pick a winner between progesterone and estradiol, because the research was never set up as a contest. Estradiol is the hormone for the heat and the dryness, the one carrying the most therapeutic power and the most risk weight, backed by guideline-level evidence for vasomotor symptoms [5] and trial evidence for vaginal atrophy [6]. Progesterone is the quieter hormone, mostly there to protect the uterine lining once estrogen enters the picture, with trial evidence behind that role [2] and an FDA-approved label to match [1], plus a real, if modest, assist with sleep [3]. If she has a uterus and estradiol is helping her symptoms, progesterone is very likely coming along with it, not as a runner-up, but as the other half of the plan. What she takes next is a conversation for her clinician, not a verdict from a scorecard, but at least now she knows which questions to bring to that appointment.
A few common questions
Is progesterone or estradiol better for hot flashes? Estradiol, clearly. The Endocrine Society guideline calls menopausal hormone therapy, with estrogen as the active agent, the most effective treatment for vasomotor symptoms [5]. Progesterone was not built for this job, so leaning on it for hot flash relief means reaching for the wrong tool.
If I take estradiol and still have my uterus, do I have to take progesterone too? In almost every case, yes. Unopposed estrogen stimulates the endometrium and can push it toward hyperplasia, a precancerous overgrowth. In the PEPI trial, cyclic micronized progesterone kept hyperplasia rates close to placebo while estrogen alone produced a marked excess [2], which is exactly why endometrial protection is an FDA-approved use of oral progesterone [1].
Does progesterone actually help with sleep, or is that just something people say? There is randomized-trial evidence behind it, with a fair caveat attached. A 2021 meta-analysis of trial data found micronized progesterone improved several sleep measures, mostly in postmenopausal women, though the effect wasn’t consistent across every measure studied [3]. It’s a modest, situation-specific benefit, not grounds for treating progesterone as a general sleep aid.
Can I just use vaginal estradiol for dryness and skip progesterone? Local vaginal estrogen is answering a different question than a systemic dose would. A Cochrane review found intravaginal estrogen relieves atrophy symptoms compared with placebo, with no clear edge among cream, tablet, or ring [6]. Whether a low-dose local product changes the need for progesterone is a judgment call for the prescribing clinician, since dose and route both factor in.
Is compounded “bioidentical” progesterone the same thing as FDA-approved Prometrium? No. Prometrium is the FDA-approved oral micronized progesterone product [1], while compounded “bioidentical” versions are not FDA-approved and aren’t reviewed by the agency for safety, effectiveness, or quality before they reach patients [7]. A compounded version can make sense for the right clinical reason, but it’s a different regulatory category, and an honest provider will tell you which one you’re actually getting.
Does progesterone cause weight gain?
Progesterone can lead to some temporary water retention for certain people, which can look like a small uptick on the scale, but the evidence for real fat gain is thin. Synthetic progestins carry a stronger link to weight changes than bioidentical progesterone does. Most clinicians see any bloating settle within the first cycle or two, as the body adjusts to the new dose.
What is progesterone actually used for in clinical practice?
Prescribers reach for progesterone for a handful of distinct reasons: protecting the uterine lining alongside estrogen therapy, supporting early pregnancy for people with a history of loss, managing irregular or absent periods, and sometimes helping sleep, thanks to its calming effect on GABA receptors. The formulation, dose, and timing shift quite a bit depending on which of those goals is driving the prescription.
What progesterone dosage is typically prescribed, and how is it determined?
There’s no one-size-fits-all number. Oral micronized progesterone for menopausal hormone therapy usually falls somewhere between 100 and 200 mg, taken at night, while luteal-phase support in fertility care can run higher under closer monitoring. A prescriber weighs lab results, symptoms, and delivery method, since vaginal and transdermal routes absorb quite differently than oral capsules do. Anyone weighing a compounded option should look for a physician-supervised pharmacy, such as FormBlends, rather than an unregulated supplement seller.
What side effects should I realistically expect when starting progesterone?
Drowsiness tends to be the most commonly reported side effect with oral progesterone, which is why most prescribers suggest taking it before bed. Some people also notice breast tenderness, mood shifts in the first week or two, or the occasional spotting if timing or dose needs fine-tuning. Serious adverse events are uncommon with bioidentical progesterone, though not impossible, so anything unusual, particularly chest pain or a severe headache, deserves a prompt call to the prescriber.
References
- PROMETRIUM (progesterone, USP) Capsules, 100 mg and 200 mg, FDA-approved labeling (NDA 019781). Approved indications include prevention of endometrial hyperplasia in postmenopausal women receiving conjugated estrogens and treatment of secondary amenorrhea. U.S. Food and Drug Administration, Drugs@FDA labeling. https://www.accessdata.fda.gov/drugsatfda_docs/label/2009/019781s013lbl.pdf
- The Writing Group for the PEPI Trial. Effects of hormone replacement therapy on endometrial histology in postmenopausal women. The Postmenopausal Estrogen/Progestin Interventions (PEPI) Trial. JAMA, 1996. Cyclic oral micronized progesterone 200 mg/day for 12 days a month kept endometrial hyperplasia rates near placebo, while unopposed estrogen produced a large excess. https://pubmed.ncbi.nlm.nih.gov/8569016/
- Nolan BJ, Liang B, Cheung AS. Efficacy of Micronized Progesterone for Sleep: A Systematic Review and Meta-analysis of Randomized Controlled Trial Data. Journal of Clinical Endocrinology & Metabolism, 2021. Micronized progesterone improved several aspects of the sleep cycle and self-reported sleep, predominantly in postmenopausal women.
- Fournier A, Berrino F, Riboli E, et al. Breast cancer risk in relation to different types of hormone replacement therapy in the E3N-EPIC cohort. International Journal of Cancer, 2005. Observational cohort; breast cancer relative risk approximately 1.4 with synthetic progestins versus approximately 0.9 with micronized progesterone.
- Stuenkel CA, Davis SR, Gompel A, et al. Treatment of Symptoms of the Menopause: An Endocrine Society Clinical Practice Guideline. Journal of Clinical Endocrinology & Metabolism, 2015. Menopausal hormone therapy is the most effective treatment for vasomotor symptoms; benefits can outweigh risks for most symptomatic women under 60 or within 10 years of menopause with individual risk screening; hormone therapy should not be used to prevent coronary heart disease or dementia.
- Lethaby A, Ayeleke RO, Roberts H. Local oestrogen for vaginal atrophy in postmenopausal women. Cochrane Database of Systematic Reviews, 2016. Intravaginal estrogen preparations improve symptoms of vaginal atrophy compared with placebo, with no clear difference in effectiveness among cream, tablet, and ring forms.
- U.S. Food and Drug Administration. Compounding and the FDA: Questions and Answers. Compounded drugs are not FDA-approved, meaning the agency does not review their safety, effectiveness, or quality before they are marketed; compounded drugs can serve important medical needs.
Written by Priya Farrell, health correspondent. Last reviewed January 2026.
For informational purposes. Any new treatment should be reviewed by a licensed professional first.